RED LEG (Conditions, Irritations & Infections)


Welcome to the turning of summer into fall! As we are encountering everything from colorful trees to colorful politicians, let’s turn our attention to the colorful legs that can sometimes be quite perplexing. Just as a red wound bed can represent different situations, so can redleg skin. In this blog post, we will concentrate on the red leg, trying to distinguish between conditions, irritations, and infections.
Hemosiderin
 The hallmark of venous insufficiency begins with H: Hemosiderin staining is that ruddy red discoloration of the skin, turning tissue a darker reddish-brown color. This staining is consistent with chronic swelling, an undeniable “tattooing” from chronic leaking of red blood cells out of capillaries and into surrounding tissue. This iron-rich staining usually starts distally, in the ankle (or gaiter) region, but can extend proximally, forming a “knee sock” pattern. It is sometimes confused with cellulitis due to its deep red appearance.
The hallmark of venous insufficiency begins with H: Hemosiderin staining is that ruddy red discoloration of the skin, turning tissue a darker reddish-brown color. This staining is consistent with chronic swelling, an undeniable “tattooing” from chronic leaking of red blood cells out of capillaries and into surrounding tissue. This iron-rich staining usually starts distally, in the ankle (or gaiter) region, but can extend proximally, forming a “knee sock” pattern. It is sometimes confused with cellulitis due to its deep red appearance.
Venous Dermatitis
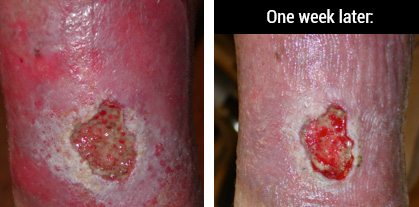 A swollen leg with or without an open wound can often present with redness and weeping in the tissues. Is this infection or irritation or both? The photo below shows a chronic wound that has been open for 3 years and had been on multiple oral antibiotics with no resolution. Her wound was also treated with topical antibiotic ointments and wrapped with kerlex. Drainage was heavy and her leg was not in any compression.
A swollen leg with or without an open wound can often present with redness and weeping in the tissues. Is this infection or irritation or both? The photo below shows a chronic wound that has been open for 3 years and had been on multiple oral antibiotics with no resolution. Her wound was also treated with topical antibiotic ointments and wrapped with kerlex. Drainage was heavy and her leg was not in any compression.
 This venous dermatitis is an irritation and inflammation of the dermal or epidermal layers that responded well to short-term topical steroids in conjunction with absorptive dressings for the wound and compression bandaging of the lower leg. The skin can be highly predisposed to contact sensitizers, so use caution with moisturizers that contain fragrance or dyes. Topical antibiotics also can exacerbate venous dermatitis and are not recommended.
This venous dermatitis is an irritation and inflammation of the dermal or epidermal layers that responded well to short-term topical steroids in conjunction with absorptive dressings for the wound and compression bandaging of the lower leg. The skin can be highly predisposed to contact sensitizers, so use caution with moisturizers that contain fragrance or dyes. Topical antibiotics also can exacerbate venous dermatitis and are not recommended.
This can also be confused with cellulitis due to its red, swollen, irritated skin.
Lipodermatosclerosis
 Venous dermatitis and long standing venous disease can progress to lipodermatosclerosis. This is characterized by an inverted champagne bottle shape of the lower leg where the proximal circumference is markedly differentiated from the distal aspect of the leg. This almost always starts with venous insufficiency.
Venous dermatitis and long standing venous disease can progress to lipodermatosclerosis. This is characterized by an inverted champagne bottle shape of the lower leg where the proximal circumference is markedly differentiated from the distal aspect of the leg. This almost always starts with venous insufficiency.
There is both an acute and chronic phase. The acute phase presents with redness, pain and inflammation, while the chronic phase is characterized by fibrotic, indurated skin that is very difficult to mobilize. The acute phase can be confused with cellulitis due to similar presentation. Usually a good history can differentiate between the two.
Lymphedema
 Lymphedema is an abnormal collection of protein-rich fluid in the skin, creating swelling (mostly in a limb). Lymphedema occurs from damage to the lymph vessels or removal of lymph nodes (secondary) or from hereditary condition where lymph vessels are absent or impaired (primary lymphedema). Chronic skin changes can occur, including increased fibrosis, poor oxygenation, and persistent edema. These skin conditions can lead to confusion with venous disease or chronic cellulitis.
Lymphedema is an abnormal collection of protein-rich fluid in the skin, creating swelling (mostly in a limb). Lymphedema occurs from damage to the lymph vessels or removal of lymph nodes (secondary) or from hereditary condition where lymph vessels are absent or impaired (primary lymphedema). Chronic skin changes can occur, including increased fibrosis, poor oxygenation, and persistent edema. These skin conditions can lead to confusion with venous disease or chronic cellulitis.
See the National Lymphedema Network for a complete discussion of this difficult condition.
Cellulitis
 So when is a red leg actually cellulitic?
So when is a red leg actually cellulitic?
The Cleveland Clinic gives a good synopsis of key points:
- Cellulitis is rarely bilateral
- Patients with cellulitis often have systemic symptoms, such as fever and leukocytosis.
- A chronic course points to a diagnosis other than cellulitis
- Plaques with a “bound-down” appearance or dark pigmentation point to a chronic disease rather than acute
- Stasis dermatitis is the most common mimic of cellulitis
CCJM 2012 Aug;79(8):547-552
The picture on the left shows a woman that has a hot, painful leg that is significantly different than her other leg (which has definite hemosiderin changes of its own). The erythema is not confined to any hemosiderin discoloration, but involves the entire lower leg and foot. She needed antibiotics immediately to treat her infection.
Dependent Rubor
 Lastly, there is a reddening or dark discoloration called rubor that occurs when a limb has poor arterial flow. When the leg is dependent, it turns dark (rubor). When elevated, the skin turns pale again (pallor). This signifies chronic limb ischemia.
Lastly, there is a reddening or dark discoloration called rubor that occurs when a limb has poor arterial flow. When the leg is dependent, it turns dark (rubor). When elevated, the skin turns pale again (pallor). This signifies chronic limb ischemia.
In those with a dark complexion, it is important to compare skin color to healthier areas. Sometimes the rubor can be mistaken for erythema that would more indicate infection. This patient has some significant ischemia in her first toe. Undoubtedly the ischemic limb will be cool to touch vs. the infected limb that would be warm or hot to palpation.
It is not always easy to differentiate a red leg with cellulitis from a red leg with hemosiderin staining, lipodermatosclerosis, venous dermatitis, or any number of skin conditions that share some of the same characteristics. Consider the treatment history and the response (or lack thereof) to antibiotics. If onset is slow and response is negligible to treatment, then consider a non-cellulitis diagnosis. Consult with dermatology and vascular to rule out various conditions.
I hope this helps you to begin to recognize and differentiate between the conditions with red legs.

This blog post was written by Robin Carlson, PT CWS
What is PT CWS? Physical Therapist and Certified Wound Specialist
Shareable Infographic
